Complete Resource and Explained in Simple Terms about Parallel bars including definition, types, gait training, indications, contraindications, precautions, patient progression and rehabilitation techniques.
Definition: Parallel bars are assistive rehabilitation devices consisting of two parallel handrails supported by vertical posts. They are used in physiotherapy to provide support, stability, and safety during standing balance training, gait training, transfer training, and lower-limb rehabilitation exercises.
Types of Parallel Bars
- Based on Adjustability
- Fixed Parallel Bars: Height and width cannot be adjusted.
- Adjustable Parallel Bars:Height and/or width can be modified according to patient needs, Suitable for patients of different ages and body sizes.
- Based on Mobility
- Stationary Parallel Bars: Permanently fixed to the floor.
- Portable Parallel Bars: Movable units with a stable base, Used in temporary treatment settings.
- Based on Design
- Standard Parallel Bars
- Pediatric Parallel Bars
- Foldable Parallel Bars
- Body-Weight Supported Parallel Bars
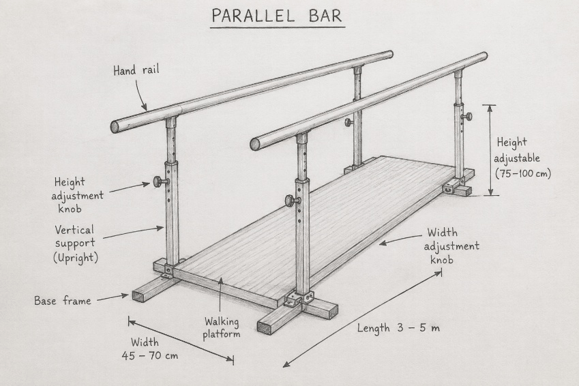
Parts of a Standard Parallel Bar
- Handrails (Bars): Two parallel rails grasped by the patient.
- Vertical Supports (Uprights): Support the handrails.
- Height Adjustment Mechanism: Allows alteration of bar height.
- Width Adjustment Mechanism: Allows modification of distance between bars.
- Base Frame: Provides stability.
- Floor Platform/Walking Surface: Area where the patient walks.
- Rubber Feet/Anchors: Prevent slipping.
Uses of Parallel Bars
- Gait training.
- Balance and coordination training.
- Standing tolerance exercises.
- Weight-shifting activities.
- Transfer training.
- Post-operative rehabilitation.
- Strengthening exercises for lower limbs.
- Neurological rehabilitation.
- Prosthetic and orthotic training.
- Early ambulation after injury or surgery.
Indications:
- Orthopedic Conditions
- Post Fractures rehabilitation
- Post Joint replacement surgery rehabilitation
- Ligament injuries rehabilitation
- Lower limb weakness training
- Neurological Conditions rehabilitation
- Stroke gait and balance training
- Spinal cord injury functional training
- Cerebral palsy rehabilitation
- Parkinson’s disease physiotherapy management
- Multiple sclerosis physiotherapy management
- Geriatric Rehabilitation
- Balance deficits physiotherapy management
- Fall prevention training
- Amputee Rehabilitation
- Prosthetic gait training
- General Deconditioning
- Muscle weakness physiotherapy management
- Prolonged bed rest recovery
Contraindications
Absolute Contraindications
- Unstable fractures without medical clearance.
- Severe cardiovascular instability.
- Acute deep vein thrombosis (DVT).
- Uncontrolled hypertension.
- Conditions where weight-bearing is prohibited.
Relative Contraindications
- Severe pain during standing.
- Marked dizziness or vertigo.
- Severe osteoporosis.
- Cognitive impairment affecting safety.
- Extreme fatigue.
Precautions
- Ensure bars are properly adjusted to patient height.
- Check stability before use.
- Use gait belt whenever necessary.
- Supervise high-risk patients.
- Monitor vital signs in medically compromised patients.
- Follow prescribed weight-bearing status.
- Remove obstacles from walking area.
- Ensure patient wears appropriate footwear.
- Stop training if pain, dizziness, or shortness of breath occurs.
Techniques of Training in Parallel Bars
A. Standing Training
Supported standing.
Static standing balance.
B. Weight-Shifting Exercises
Side-to-side shifting.
Forward-backward shifting.
C. Gait Training
Step-to gait.
Step-through gait.
Reciprocal gait.
Heel-toe walking.
D. Balance Training
Single-leg standing.
Tandem standing.
Dynamic balance activities.
E. Transfer Training
Sit-to-stand.
Stand-to-sit.
F. Prosthetic Training
Weight acceptance.
Equal weight distribution.
Prosthetic gait practice.
G. Functional Activities
Turning.
Reaching activities.
Obstacle negotiation (advanced stage).
Standard Parallel Bar
Typical Dimensions:
Length : 3–5 m (10–16 ft)
Width : 45–70 cm
Height : 75–100 cm (adjustable)
Standard Positioning
Height of bars: approximately at the level of the patient’s greater trochanter or wrist crease when standing upright with elbows flexed about 20–30°.
Width: allows comfortable standing and walking without excessive shoulder abduction.
Click to get All Therapeutic Exercise Notes
Click to get all Electrotherapy Notes
References:
Kisner & Colby: Therapeutic Exercise: Foundations and Techniques.
O’Sullivan & Schmitz: Physical Rehabilitation.
Dena Gardiner: The Principles of Exercise Therapy.
Braddom: Physical Medicine and Rehabilitation.
For more notes click on: www.physiotherapyphd.com
